Moving Beyond the Cost Pyramid

How one-size-fits-one engagement can transform value-based population health
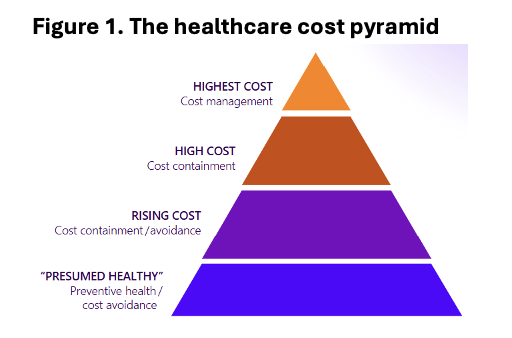
Healthcare’s Cost Pyramid (Figure 1) has served as a useful tool for understanding how cost management, containment and avoidance strategies should be applied to different populations. At the base of the pyramid lies the 50% of the population that accounts for only 3% of health spending, followed by rising-cost and high-cost populations.
But it is the top of the pyramid, and the well-understood statistic it represents, that consistently receives the most attention:
For any large insurance population in the U.S., the sickest 5% of the population accounts for approximately 50% of the healthcare spending.
Whenever decision makers are examining ways to reduce healthcare spending, this fact tends to dominate the conversation.
The current thinking goes something like this, “Improving the efficiency and quality of care of the sickest 5% of the population should be the most efficient way to significantly decrease healthcare spending overall.”
After all, 5% should be a “manageable” population and the potential savings should be substantial. All that’s required is to invest in disease management programs that target the “Five-Percenters”, and the savings will automatically materialize.
Unfortunately, the many attempts to leverage this “Five-Percent Strategy” by committing extra resources, time and effort to impact such a small portion of the overall population has not played out in practice. In fact, despite the significant investment focus on this segment, the average engagement rate across high-risk groups is below 30%, and 60% of members contacted by care management fail to adhere to recommended care plans.
Why is this the case?
Four Fallacies About High-Cost Populations
Unexamined assumptions are dangerous for any business sector. The Five-Percent Strategy has been ineffective because it’s based on four erroneous assumptions about the top tier of Healthcare’s Cost Pyramid.
1) The Homogeneity Misnomer
Assumption: Because the Five-Percent population is so small, with little turnover year after year, it must be homogenous and share a basic set of medical conditions.
Fact: About two-thirds of the Five-Percent Population changes unpredictably each year. In a population with such high turnover, simply knowing who the highest-cost members today is not an accurate predictor of future risk. High cost does not always equal highest ongoing risk. Managing risk effectively requires identifying who is most likely to become a Five-Percenter in the future.
2) The Impact Fantasy
Assumption: Because the Five-Percent population is a known quantity, it should be easy to make a positive impact.
Fact: Because Five-Percenters are a changing population, about two-thirds of the high-cost dollars spent on them are not clinically effective. This explains why many disease-management programs haven’t delivered positive returns.
3) The Primary Care Prejudice
Assumption: Once primary care identifies a medical condition, it should be easy to enroll patients in the right program to address the issue and improve their health. Example: ‘We identified 2,000 diabetics. Let’s get them to the top of the call list for our diabetes management program.’
Fact: Nearly all of the Five-Percenters have multiple conditions that may impede their ability or willingness to enroll. Focusing on just one condition doesn’t address the inter-related medical complexities that require a whole-person, personalized approach.
4) The Myth of Easy Adherence
Assumption: Five-Percenters will adhere to their next steps in care once we connect them with the right resources and make sure they are enrolled in the right program.
Fact: Studies* show that a substantial portion of high-cost patients live in disadvantaged neighborhoods and face Social Determinants of Health (SDoH) barriers (e.g., low income, housing or food instability) that interfere with their ability to follow care plans.
Moving beyond the cost pyramid
With these four fallacies revealed, a new imperative becomes clear. To significantly reduce healthcare costs, health plans need to move beyond the traditional cost-saving strategy focused on the top tier of the Cost Pyramid. What’s needed is a new operational model, a more comprehensive approach based on the following three shifts in strategy.
1) Move from a Basic Accounting (HCC Coding) Strategy to a Rising-Risk Strategy
When two-thirds of the highest-cost population changes from year to year, a simple acocunting of who is in the top tier is perpetually out of date. The most critical piece of data is not who the Five-Percenters are now, but which members are most likely to become Five-Percenters in the future. To implement this “Risking-Risk Strategy” and accurately determine the most likely "Cost Bloomers,” health plans need to make a second strategic shift.
2) Move from a Retrospective to a Predictive Model
The traditional care management model looks backwards. It analyzes past claims and data and then attempts to make interventions based on what has already occurred. To identify “Cost Bloomers” requires augmenting the retrospective approach with a new predictive and prescriptive models. This aspect of the “Rising-Risk Strategy” utilizes advanced algorithms and machine learning to analyze entire populations and predict future outcomes based on patterns available in existing data, including the estimated 97% of health data that is currently unused.
3) Move from a One-Size-Fits-All Engagement Model to a One-Size-Fits-One
Once the “Risking-Risk” population has been identified, engaging with these members as effectively as possible is now the goal. Member engagement strategies need to leverage Generative AI (GenAI) and make every communication and interaction personalized and tailored to the needs of each member. This requires a holistic understanding of the needs and preferences of each member. New data elements that measure consumer preferences, behavioral patterns of engagement, social relations (strength of their support system) and SDoH factors can contribute significantly to this understanding and ultimately, improve the health outcomes we seek to achieve.
A New Strategy for Value-Based Care
Attempts to drive down costs by focusing on the top tier of Healthcare’s Cost Pyramid have not yielded the desired results. While continuing interventions that close gaps in care, improve medication adherence and reduce hospitalizations and readmissions are important, health plans need to adopt a Rising-Risk Strategy that identifies the rising-risk population and then de-risks this population through proactive, personalized engagement. With this new strategy, each member is more motivated and informed to take the necessary actions that not only improve population health but also finally bend the cost curve.
FAQs
-
Because the high-cost population changes significantly year over year, making it difficult to sustainably impact costs through disease management alone.
-
It assumes high-cost members are stable, easy to impact, and likely to adhere to care plans, which has proven inaccurate in real-world practice.
-
Many high-cost members have multiple conditions and face Social Determinants of Health barriers that limit enrollment, adherence, and sustained engagement.
-
A Rising-Risk Strategy focuses on identifying members likely to become high-cost in the future and intervening earlier with predictive models and personalized engagement.
-
By shifting from retrospective analysis to predictive models and using personalized, AI-driven engagement to proactively reduce future risk and costs.
*Agency for Healthcare Research and Quality. n.d. Management of High‑Need, High‑Cost Patients. NCBI Bookshelf, National Center for Biotechnology Information. Accessed July 31, 2025. https://www.ncbi.nlm.nih.gov/books/NBK575195/.LeBreton, Maribeth S., and Eileen Sosa. “High‑Need, High‑Cost Patients and Social Determinants of Health.” JLGH: Journal of Lancaster General Health 15, no. 4 (Winter 2020). JLGH.org. Accessed July 31, 2025. https://www.jlgh.org/Past‑Issues/Volume‑15‑Issue‑4/LeBreton_High‑Need‑High‑Cost.aspx.